

Faecal ‘poop’ transplantation may seem a bit gross, but the use of this peculiar method in the treatment of deadly recurrent Clostridium difficile infection has shed miraculous results compared to standard antibiotic therapy. Let’s find out why poop is so more effective than antibiotics at treating this bacterial infection!
Clostridium difficile (C. difficile) is a bacteria which causes severe diarrhoea and colitis — inflammation of the colon. It is estimated to affect around half a million individuals yearly in the US, with mortality rates being as high as 40% in hospitalised patients.
A large problem with C. difficile infection (CDI) stems from its treatment: CDI is managed with strong courses of antibiotics, mostly with vancomycin.
So, what’s wrong in giving antibiotics to treat a bacterial infection?
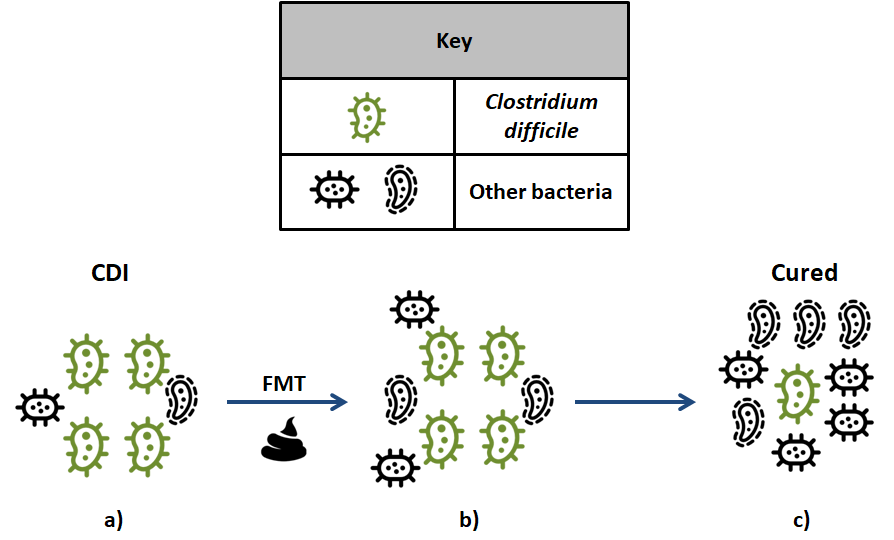
You see, C. difficile is actually present in all of us, but the large diversity of bacteria (known as the microbiota) living within our gut prevents it to thrive.
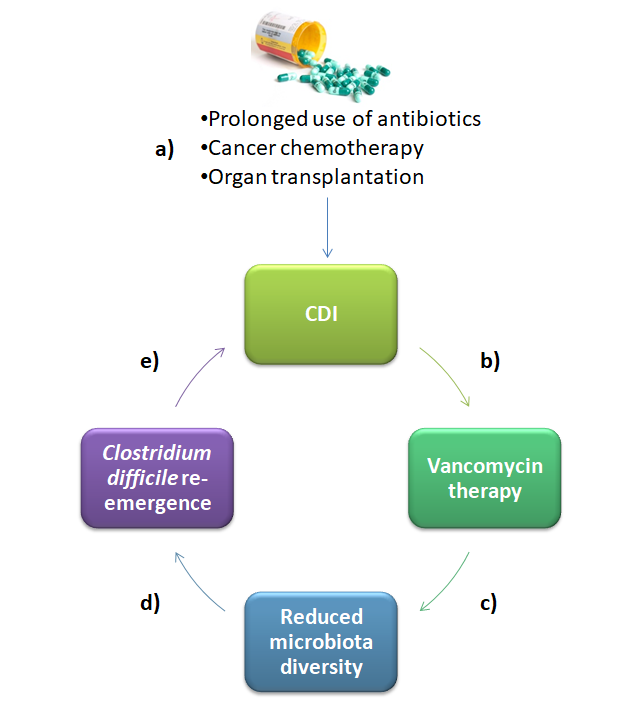
Unfortunately, individuals treated with long courses of antibiotics or those receiving chemotherapy experience large reductions in their microbiota diversity, which in some instances allows C. difficile to colonise their gut and cause disease.
Using antibiotics to fight off CDI is problematic because you are also killing off good bacteria, which will further disrupt the delicate balance of the microbiota and possibly allow C. difficile to counterattack.
While vancomycin can effectively get rid of C. difficile in individuals who have just been diagnosed, around 35% of patients suffer recurrent infection, which is when it becomes clear that antibiotics are doing more harm than good.
And guess how recurrent CDI is treated?
Exactly in the same way — By giving more antibiotics.
Unfortunately, the efficacy of continuously giving vancomycin to patients with recurrent CDI is very low, with a cure rate of just 30%!
Doing this repeatedly further weakens the microbiota and makes C. difficile recurrences more likely.
Instead of disrupting the microbiota, a cure should strive to restore it!
This is achievable using a technique known as FMT, which stands for faecal microbiota transplantation.
In FMT, the faeces of a healthy donor are diluted with saline, blended and subsequently inserted into the colon of the affected individual. Within hours, the healthy bacteria from the donor’s faeces take over the microbiota of the infected individual, competing for nutrients with C. difficile and drastically reducing their numbers, which may potentially cure CDI.
‘Poop’ transplantation may seem crazy and hard to believe, so I have chosen to analyse a study which compared the efficacy of FMT with that of the antibiotic vancomycin in treating recurrent CDI. The results were fascinating so let us explore them now.
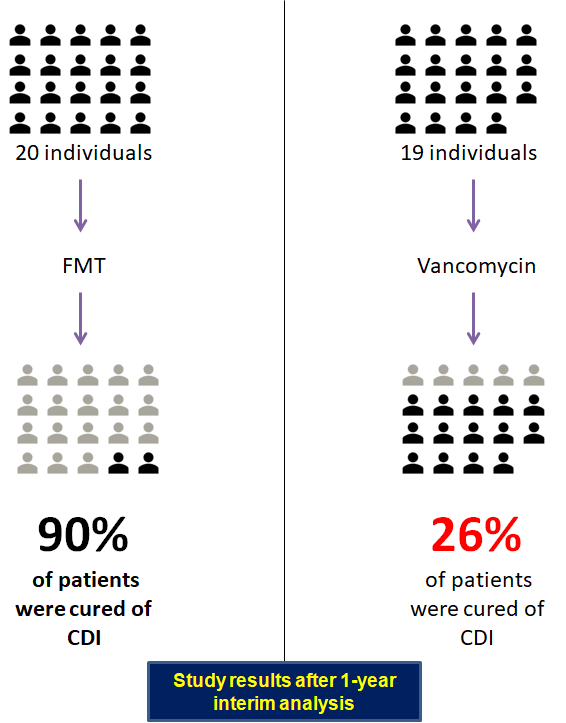
In this open-label randomised controlled study, 39 participants who had experienced recurrent CDI on one or more courses of specific antibiotics were recruited and divided into two treatment protocols: 20 subjects were assigned to the FMT group and 19 were placed in the vancomycin intervention.
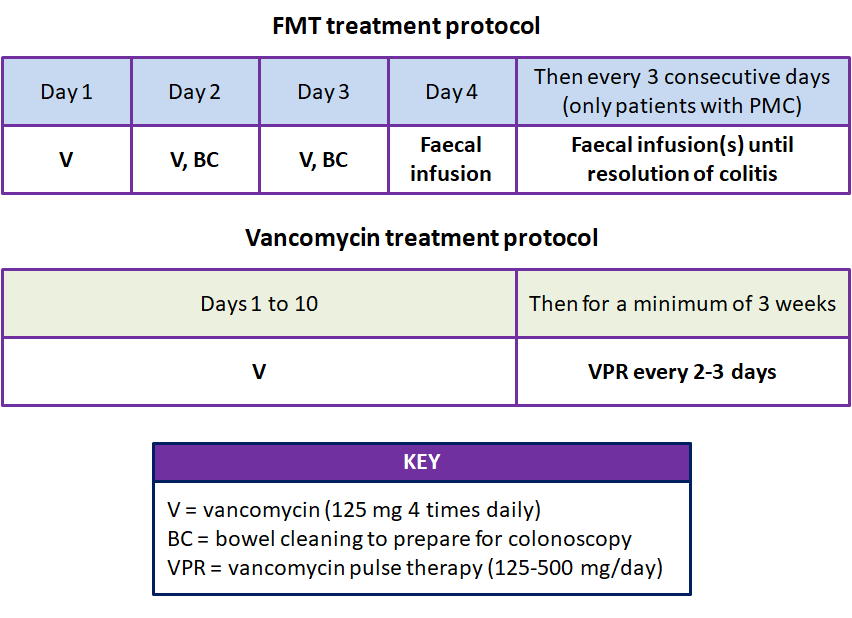
Individuals in the FMT group were given a short course of vancomycin for 3 days, with bowel cleaning taking place on the last two days of antibiotic use. On the 4th day patients underwent FMT via colonoscopy.
Meanwhile, individuals in the vancomycin group were given a standard course of the antibiotic for 10 days, followed by a pulse regimen (125–500 mg once-daily every 2–3 days) for at least 3 weeks.
FMT-treated patients who developed recurrent CDI after the first faecal transplant were to be given a second infusion of faeces within 1 week. However, this part of the protocol was later modified, with repeated faecal infusions given every 3 days to all patients with pseudomembranous colitis (PMC), until the resolution of colitis.
In case you wondered, PMC refers to inflammation of the colon as a result of toxins produced by C. difficile. Not all patients with CDI develop PMC, but those with it experience more severe disease.
With this being clear, let’s looks at the results!
Overall, FMT was shown to be extremely effective, with 90% (18/20) of patients being cured of CDI, compared to a success rate of 26% (5/19) in the vancomycin group.
The results revealed an overwhelming superiority of FMT over using antibiotics when treating recurrent CDI. However, by dissecting the data further there are more obvious differences and fascinating results too, so let me explain them…
In the FMT group, 65% (13/20) of patients were cured after just one faecal transplant. It’s worth highlighting that all of the patients who were cured on the first try did not have PMC.
Meanwhile, 5 out of 7 patients with PMC were cured with repeated faecal infusions. Of these 5 cured patients, 3 received 2 faecal infusions, 1 patient received 3 infusion; and 1 patient underwent 4 infusions.
Interestingly enough, the two PMC patients who were not cured with FMT were the first ones to be treated. These two patients suffered recurrent CDI and later died from C. difficile-associated clinical complications, being regarded as treatment failures.
However, these two patients had PMC and were treated with the old protocol…
This is when the researchers realised that something was not working quite right and they decided to amend their protocol to provide regular faecal infusions to PMC patients until their colitis resolved.
Quite remarkably, after the protocol was amended the success rate of FMT was 100%, with 18/18 patients being cured of CDI!
In addition to its impressive efficacy, FMT was very safe.
While most patients experienced diarrhoea, abdominal cramping and bloating following faecal infusions, these symptoms disappeared within 12 hours. Interestingly, no patients expressed any concerns about FMT or refused treatment.
Overall, this study clearly revealed that the use of FMT via colonoscopy was significantly better at curing CDI compared to vancomycin. Moreover, the researchers were able to highlight that patients with PMC require several and frequent faecal infusions to be cured from CDI, whereas those without this complication are cured with a single shot.
To sum up, FMT restores the damaged microbiota of patients suffering from recurrent CDI, showing unprecedented efficacy outcomes compared to conventional vancomycin antibiotic therapy, and calling for an urgent change in how we treat this fatal bacterial infection.









